The Nipah Virus Outbreak: Everything You Need to Know About India’s New Epidemic
Photo by Chris Jackson/Getty Politics Features Nipah Virus
At least 40 people have been infected and 13 have died in southern India in an outbreak of Nipah, a rare and deadly virus with no known cure. That’s not a large outbreak, but it’s enough that epidemiologists have raised concerns about a possible global health emergency. Nipah is on the World Health Organization’s list of priority emerging diseases with epidemic potential, a list that also includes Ebola and Zika. On Monday the Hindu Times reported the first suspected case of Nipah to be found outside the virus’s origin in the state of Kerala, in a young man who traveled by train to Goa.
There’s a lot to worry about these days. Should epidemics be one of them?
In a word, yes. Should this particular epidemic be one of them? If you live in the U.S., not yet, but even though it’s improbable that Nipah will infect great numbers of people outside southern India, it’s not impossible. And earlier this month health officials in the Democratic Republic of Congo declared a new Ebola outbreak, which has now spread from its rural origins to an urban center.
At some point everybody dies. The question a pandemic raises is if a whole lot of us will die at the same time. The answer, sadly, is that we will. But don’t despair! Yet! Here’s what you need to know about the recent outbreaks of Nipah and Ebola, and what the U.S. government is planning to do about the risk of a future global epidemic.
What’s Nipah and how is it spread?
Nipah virus (NiV) is a zoonotic virus that causes severe disease animals and humans. (A zoonotic virus is a virus that can be transmitted from animals to humans, such as rabies or zika.) On the scale of viruses, NiV is relatively new. It was first identified in the Malaysian town of Nipah in 1998, and subsequent outbreaks have been more or less contained to South and Southeast Asia, most notably Bangladesh, where in 2004 a number of people contracted the virus after consuming contaminated date palm sap. A closely related virus called Hendra first appeared in Australian racehorses in the mid-nineties.
NiV can present as severe respiratory infection, extreme fevers, convulsions, vomiting, and often a swelling of the brain, called encephalitis. There’s no known cure and no vaccine, though researchers are working on one. The virus’s primary hosts are fruit bats, which can transmit the disease directly to humans through the vectors of bites and scratches, or via contaminated food and water. Other animals, such as pigs, can also contract the virus and transmit it to people.
And as this recent outbreak shows, NiV can also be transmitted from humans to humans through bodily fluids, though the virus doesn’t currently have an airborne vector. The WHO reports NiV has mortality rates of up to 75%, though the recent strain to appear in India seems less deadly than that. Last week a nurse who had been caring for infected people in an Indian hospital contracted the infection. From her hospital bed she wrote her husband, “I think I am almost on my way. I may not be able to see you again. Sorry. Take care of our children. Lots of love.” She died Monday.
As of this writing, Indian health officials haven’t tracked this outbreak to a host. The first three people to get infected belonged to a family, and officials first suspected they’d contracted the disease from the family well, where they’d found dead bats in the water. Those weren’t fruit bats, however, and ultimately they tested negative. Officials have warned people in southern India not to eat any fruit that has bite or scratch marks, and they’re now testing every Tom, Dick, and Harry in the area, as well as livestock and pets.
Thirteen people? Why is this making international news?
Well, it’s not exactly a slow news cycle. Though the reaction might seem alarmist, the experts say there’s good reason to be concerned. Stephen Luby, an epidemiologist at Stanford, explains: “It is conceivable that there is currently a strain of Nipah virus circulating among bats that, if it infected people, would efficiently transmit from person to person. So far,” he adds, “we have not identified such a strain.”
Luby says one worry is that the virus could mutate into a strain that concentrates in the respiratory tract, which would increase the risk of airborne transmission. He comfortingly points out that the risk of this specific mutation isn’t exactly a random event, because “anytime a virus infects a human, it is in an environment that selects for survival in that context.”
I’ll emphasize again that although this disease is a real and emerging global threat, the outbreak in Kerala so far seems localized, with minimal vectors of transmission. This recalls the 2014-2016 Ebola outbreak in West Africa, which, though the disease spread only through contact with bodily fluids, killed 11,000 people. And that’s thanks to a major international effort, led mostly by the United States, which eventually managed to isolate the disease before it could spread through major urban areas. Speaking of Ebola, though, there’s just been another outbreak in the Democratic Republic of Congo, and this time cases have been documented in an urban area on a river that serves as a major shipping and travel corridor.
If you don’t live in these regions and you’re not a health official, you probably shouldn’t lose sleep over the threats from these two outbreaks. But even if you’re not, you should have a healthy concern about the prospect of a global epidemic.
Pandemic!
Whenever I read up on this stuff I freak out for a day or two, but it eventually disappears, and usually long before the epidemic that got me thinking about it in the first place. That’s understandable because the idea of pandemic is so alien to our time, so abstract, that it seems nonexistent. But that’s not the right way to think about it, because if the entirety of human history is any guide, everyone reading this today is likely to experience a major and deadly global epidemic in their lifetime. And public health experts are quick to remind us that, considering the circumstances and trends of modern civilization, whatever that epidemic is would very likely be one of the worst in history. Oxford University’s Global Priorities Project lists pandemic as one of the most catastrophic threats we face today. That’s the truth, and we need to adapt to it. But the way the world has been developing, we’re actually compounding the risk.
Jimmy Whitworth, a professor of international public health at the London School of Hygiene and Tropical Medicine, summed up the core problem to CNN: “We’re only as secure in the world as the weakest country.”
In this day and age, that’s not really secure.
A few specific factors compound this general problem, among them urbanization, international travel, conflict, wealth, and climate change. We’re all aware how interconnected we’ve become, with goods and people traveling faster, over longer distances, and more frequently than ever. So we’re going more places, but at the same time we’re also clustering closer together. Between 1990 and 2014 the number of megacities (pop. 10 million or higher) nearly tripled, going from 10 to 28, and the U.N. has predicted that by 2050 two out of three people will be living in urban areas.
So in terms of pandemic, you can think of this like we’re shooting more and more flaming arrows at bigger, gasoline-soaked targets.
Further, as we create new places to accommodate this growing population, people will move into new environments, where they’ll interact with new animals and, subsequently, new diseases. The mass migrations of climate refugees will add to this problem.
Speaking of climate change, pathologists have raised the possibility that warmer temperatures could release ancient viruses and bacteria that have been frozen in tundra or ice, unseen for centuries or even longer. Humans would have virtually no natural immunity to these diseases, should they emerge and spread.
Many of the exacerbating factors arise out of social conditions in poor and/or unstable countries. Most of those 18 new megacities have appeared in the developing world, for instance. The developing world is also home to some of the places that will experience the first major social consequences of climate change. In Bangladesh, for instance, which has seen several Nipah outbreaks, a sea level rise of three feet would put nearly 20 percent of the land underwater and displace more than 30 million people.
Countries experiencing armed conflicts are highly vulnerable . An outbreak in Yemen or Syria, for instance, would devastate that country. On top of that, it seems pretty hopeless that a serious outbreak could be contained at all in such a place. It’s a terrible irony that the places that need the most help get the least. Many countries in subsaharan Africa, for instance, can’t afford to develop or maintain modern infrastructure that would allow health workers to get quickly to the site of an outbreak. Developing countries, as well as countries experiencing conflict or those under unstable political circumstances, unsurprisingly also don’t attract a whole lot of doctors and nurses. In fact, most leave.
The result is that if and when diseases break out in these areas, it takes health officials a long time to trace the virus, as well as to treat victims and quarantine the “rings” of people at risk of exposure. This not only gives diseases more time to spread, it gives them more chances to mutate into strains that can move easily between humans. So far we’ve been able to contain these outbreaks, such as the 2014 Ebola outbreak in West Africa, which, though it killed 11,000 people and made it to the United States, could have been much worse.
Poor, hot, crowded, and unstable. As these dimensions of our society increase, so does the risk and severity of epidemic.
So what are we doing about it?
Public health experts have been ringing the alarm about the serious threat of global pandemic for years. Over the last four years of the Obama administration the CDC received an annual funding increase of $52 million for studying emerging and zoonotic diseases, which pose the highest epidemic threat. But we have a new presidential administration that either doesn’t understand or doesn’t believe the seriousness of that risk, and which has cut that same funding by about $59 million.
Trump’s first budget would have cut funding for the Department of Health and Human Services by more than $15 billion. This most specifically includes major cuts at the National Institutes of Health, which subsidizes more research on infectious diseases than any other agency in the world. Trump also cut funding for the State Department and foreign aid, which both play critical roles in stopping the spread of diseases overseas.
And it took Trump about a year and a half to install his head of the CDC, Dr. Robert Redfield, a homophobic zealot who, among other things, once wrote the introduction to a book that called AIDS “God’s judgment.”
Science!
But perhaps we can look to Trump’s tough tweets on what he perceived as Obama’s weak Ebola response. Trump authored a total of 100 tweets on the subject of Ebola, most of them in a xenophobic frenzy in fall of 2014. The future president, of course, was a strong advocate for a travel ban from West African countries to the United States. (He also happens to be a vile racist.) So Trump understands the need for quarantine, but he doesn’t understand the critical role the United States plays in helping other countries quarantine and treat infections at the local level. He also, you’ll be shocked to learn, doesn’t understand how diseases work.
?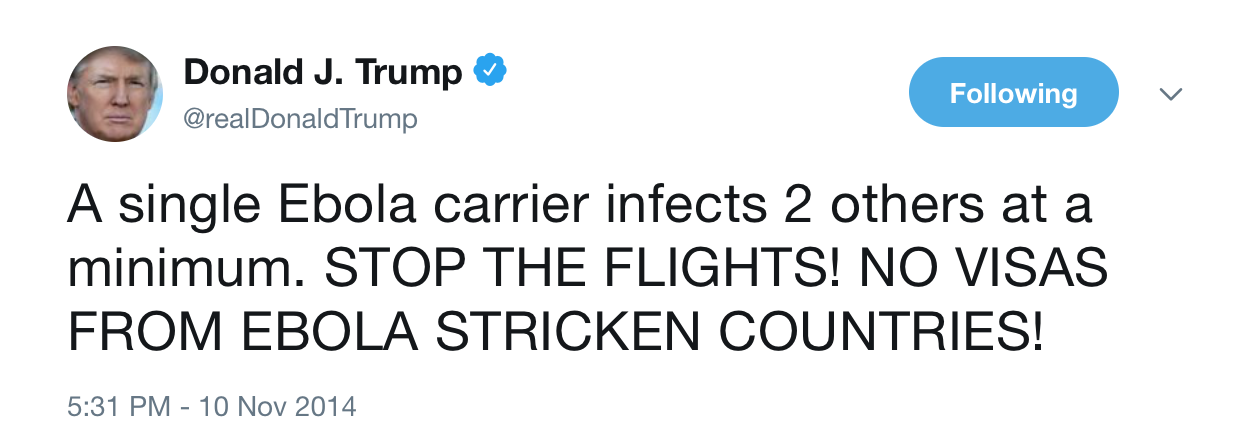
A single Ebola carrier doesn’t automatically infect two other people at minimum. If that were true, we’d all have been seriously ill or killed. Ebola carriers infect people who come into contact with their bodily fluid. What Trump conflates here is that if on average one carrier does infect two people, that sets the stage for a global pandemic. And that’s a real risk: In the case of Ebola in 2014, 3% of carriers were responsible for 61% of infections.
Now imagine that virus traveled through the air. Nothing short of automatically sealing off all forms of travel and trade into and out of the country, to any other country, would be any help. Not only is that impossible, but if that’s our big plan, we’re only setting ourselves up for a disaster. An infection that kills 13 people might not seem like such a threat right now, but everything has to start somewhere. If we neglect our moral and political duty to the rest of the world, we’ll pay for it. If we don’t fight it there, we’re going to have to fight it here.
So if you’re like the rest of world and feel less and less like you can depend on the U.S. government, here’s how to survive an epidemic. Gesundheit!